Access CE Certificate/Transcript
To view your CE credits and download your CE certificate/transcript, please log in with your username and password at: https://cme.smhs.gwu.edu/my/acivities/
If you need to reset your password, select "Request New Password" to receive instructions via email.
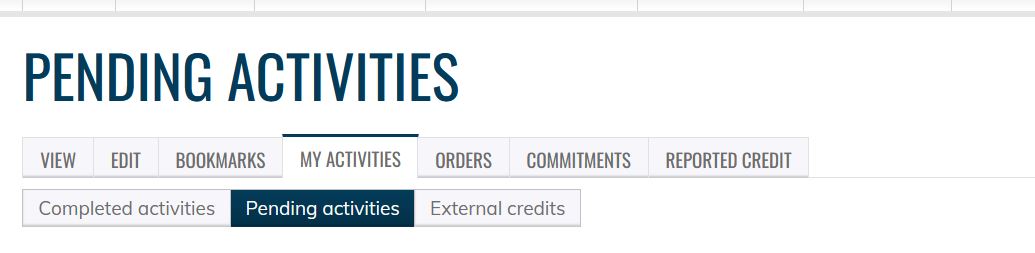
Important: If you do not see an activity listed, please check your Pending Activities to ensure you have completed all activity requirements.
CPE Credits (Pharmacists Only)
As an ACPE-accredited provider, GW is required to report all CE credits within 60 days of the learner's completion of the activity. To comply with this requirement, CEHP typically reports all CE credits on the last Friday of each month.
Please check your NABP profile within 2-3 days after the last Friday of the month to verify that your credits have been successfully submitted to NABP.
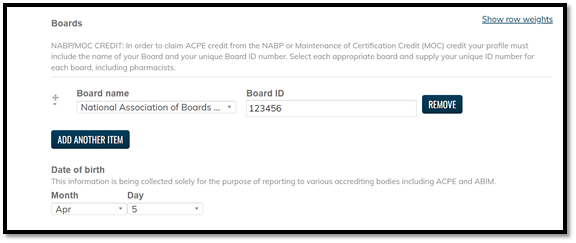
If you do not see your credits, please check your EthosCE learner account to ensure that you have selected National Association of Boards of Pharmacy from the dropdown menu and have entered your NABP ID and date of birth.